92% of executives at self-funded health systems say their employee health plan is successful, but 35% are actively re-evaluating whether their approach to keeping care in-system is still the right balance.
A growing number of large U.S. health systems have made a strategic bet: self-fund employee health coverage and steer care into their own networks. The logic is straightforward. Costs stay contained. Care stays coordinated. And the system captures revenue it would otherwise send to outside providers.
What isn’t settled is how to run it well. In a new study commissioned by Brighton Health Plan Solutions, 250 C-level executives at large, self-funded health systems said their plans are successful by wide margins, but a significant share acknowledged the balance between domestic utilization and employee flexibility is getting harder to hold. Meanwhile, a parallel survey of 352 health system employees revealed that while most are satisfied with their coverage, the administrative experience behind it, billing, claims, referrals, exceptions, is where trust erodes.
The question this study answers isn’t whether self-funded, system-directed health plans work. They do. It’s whether health systems have the right administrative partner to make them work well for everyone.
Purpose of this study
Brighton Health Plan Solutions commissioned the 2026 Self-Funded Health System Benefits Report to measure how self-funded, system-directed employee health plans are performing from both perspectives: leadership strategy and employee experience. The research included two parallel surveys conducted in March 2026: a Censuswide survey of 250 U.S. C-level executives at large, multi-site health systems (1,000+ employees) with self-funded plans, and a Pollfish survey of 352 employees at health systems of comparable size.
Among the executives surveyed, 42% operate in-system networks where care is primarily delivered within their own health system, 36% use tiered or preferred networks where their providers are favored but external options exist, and 22% offer broad or open networks. That range of plan designs allows a direct comparison of how network restrictiveness shapes leadership priorities, employee experience, and the demands placed on the third-party administrator
Key findings of the 2026 Self-Funded Health System Benefits Report
- 92% of executives at self-funded health systems rate their employee health plan as successful: Over half (52%) said very successful. Just 2% rated their plan unsuccessful. Confidence runs high, but it isn’t unconditional.
- 35% of executives are actively re-evaluating the balance between domestic utilization and employee choice: Among in-system network leaders, this rises to 42%, even as 56% of those same executives say strong utilization is essential. The tension between conviction and reconsideration is sharpest where the networks are most restrictive.
- 54% say administrative flexibility is critical to making self-funded plans work: Executives rated flexibility for exceptions, referrals, and navigation support as critical to employee trust and satisfaction. Among broad/open network leaders, that figure climbs to 69%.
- 99% of executives say the TPA is important to overall plan performance: 59% called it very important, and 16% said mission-critical. In broad/open networks, 24% rated the TPA as mission-critical, more than double the rate among in-system executives (11%).
- Executives and employees disagree on where friction lives: Executives ranked privacy concerns as the #1 source of friction (38%). Employees ranked it last (5%). Employees’ top complaint, unexpected out-of-pocket costs (37%), barely registered on the executive list.
- Only 54% of employees are confident plan decisions serve their best interests: While 78% say they’re satisfied overall, the 24-point gap between satisfaction and trust suggests many view their self-funded plan as “good enough” rather than genuinely employee-centered.
- Nearly half of employees feel caught between their employer’s two roles: 49% say they at least sometimes feel tension between their employer’s role as a healthcare provider and as their insurer, rising to 52% in restricted-network plans.
“The fact that nearly 4 in 5 employees are satisfied tells us the fundamental model works,” said Michelle Zettergren, President, Chief Sales and Marketing Officer at Brighton Health Plan Solutions. “But when you look at the trust and confidence data, it’s clear there’s a gap between a plan that employees tolerate and one they actually believe is working for them. That gap is an administrative problem, and it’s solvable.”
The utilization balancing act
The defining challenge of self-funded health system plans is domestic utilization: how tightly to steer employees into the system’s own providers. The executive data shows an industry caught between commitment and doubt.
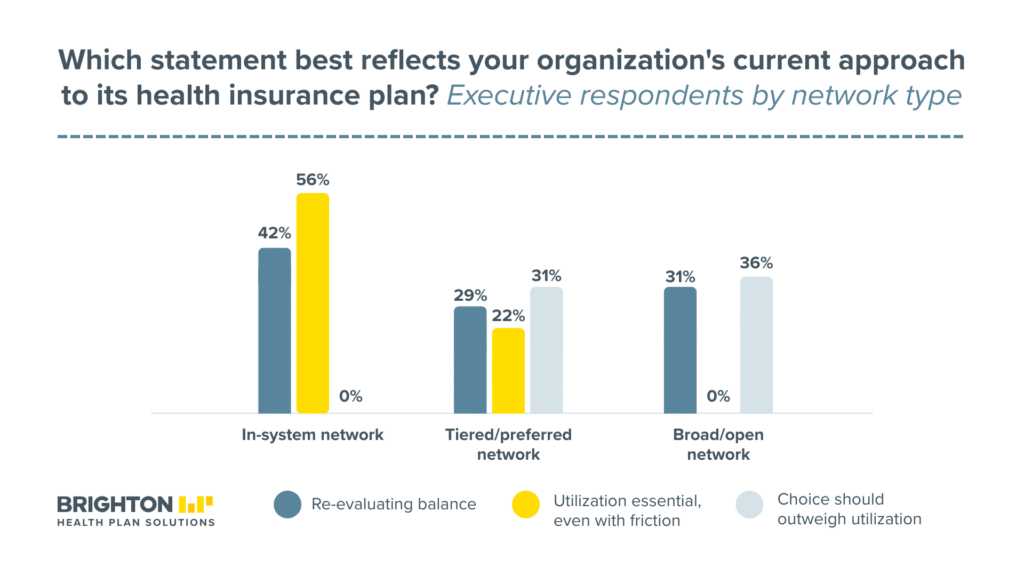
Among all executives, 32% said strong domestic utilization is essential even if it creates some employee friction. 19% said employee choice and flexibility should outweigh utilization. 14% called for a balance. And 35%, the largest single group, said they’re actively re-evaluating.
The network-type breakdown makes this sharper. Among in-system network executives, the responses split almost evenly: 56% said strong utilization is essential even if it creates friction, while 42% said they’re actively re-evaluating. Not a single in-system executive said employee choice should outweigh utilization. These are leaders deeply committed to the model, but nearly half are questioning how it’s currently balanced.
At the other end, broad/open network executives look completely different. None said strong utilization is essential. 36% said employee choice should come first. And 31% are re-evaluating, which for open-network leaders means considering whether they should be steering care more aggressively, not less.
For tiered/preferred network leaders, the middle ground, 29% are re-evaluating and 31% said choice should outweigh utilization. Only 22% held firm on strong utilization.
The takeaway: regardless of where a health system currently sits on the network spectrum, a third or more of its leadership is actively questioning the trade-offs. That’s an industry at an inflection point, and it puts enormous pressure on the administrative infrastructure to deliver flexibility without sacrificing the financial benefits of the self-funded model.
What executives see vs. what employees feel
The dual-survey design reveals a calibration problem. Executives aren’t unaware of friction in their self-funded plans. They just misjudge where it hits hardest.
Only 26% of executives said they receive generally positive feedback with few recurring complaints. The rest reported hearing about confusion with coverage or claims (21%), concerns about limited flexibility (21%), difficulty accessing providers (16%), and rising employee costs (15%). The picture varies by network type: in-system leaders hear the most about provider access issues (20%), while tiered/preferred leaders hear about confusion (27%) and flexibility concerns (27%) at higher rates.
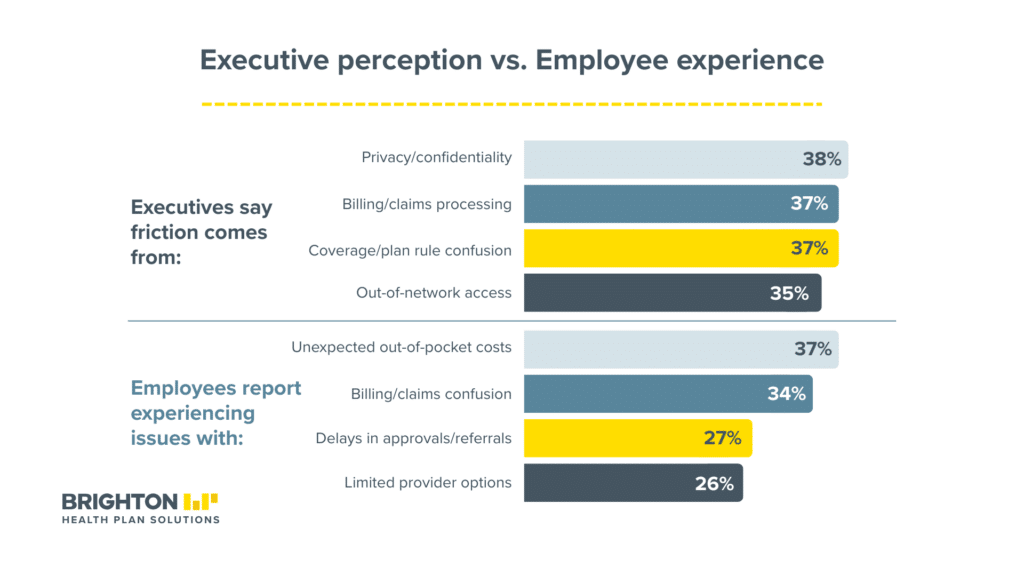
When asked where friction arises, executives pointed to privacy and confidentiality concerns (38%), billing and claims processing (37%), and coverage confusion (37%). In-system leaders were most likely to cite privacy (41%) and billing (40%) as top friction sources.
Employees told a different story. Their most commonly experienced problems: unexpected out-of-pocket costs (37%), billing or claims confusion (34%), delays in approvals or referrals (27%), and limited provider options (26%). Privacy, the executives’ top concern, ranked last at 5%.
The mismatch matters because it shapes where leaders direct improvement efforts. If executives overvalue privacy and undervalue the financial sting of unexpected costs, they may invest in the wrong administrative fixes.
The employee experience: satisfied but skeptical
Beneath the executive confidence, employee data tells a more nuanced story. 78% of employees at these self-funded health systems said they’re satisfied with their plan. A third said very satisfied. When compared to other plans they’ve had, half said this one is better.
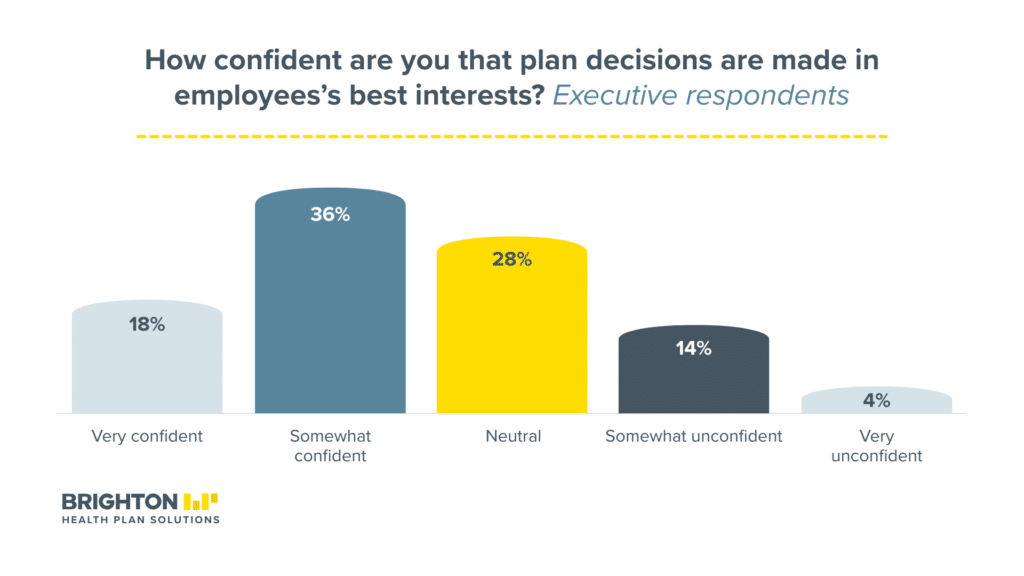
But satisfaction doesn’t equal trust. Only 18% of employees said they’re very confident that plan decisions are made in their best interest. Another 36% said somewhat confident. And 28% landed in neutral. In open-network plans, 70% expressed confidence. In fully restricted plans, that dropped to 49%.
Administrative friction is where the experience breaks down. 27% of employees said admin issues cause frustration often or very often, rising to 30% in fully restricted plans versus 16% in open networks. And 49% of employees said they at least sometimes feel caught between their employer’s role as a care provider and their role as an insurer, with that tension climbing to 52% in restricted plans.
When asked what their plan feels like in practice, 20% of employees said it feels designed more around the system’s goals than their own needs, rising to 24% among those in the most restricted plans. 35% said it works for both sides. 37% said mostly fair even if restrictive.
The single biggest improvement employees wanted: lower costs (41%). Second: more flexibility outside the system (25%). Only 11% said the plan works well as-is.
Where the TPA fits in
If the industry is re-evaluating its utilization approach, the third-party administrator is where that re-evaluation lands operationally. And the executive data makes clear that leaders already see the TPA as central to plan performance.
99% of executives said the TPA is important. But importance takes different shapes depending on the plan. Among broad/open network executives, 24% rated the TPA as mission-critical, more than double the 11% among in-system leaders. That gap reflects what open-network plans demand: with employees spread across more providers and more care settings, the TPA has to navigate complexity that in-system plans partially avoid through restriction.
The capabilities executives want from a TPA also shift by network type. In-system leaders prioritized experience administering health system-run or provider-sponsored plans (31%) and data transparency and reporting (30%). Broad/open network leaders put care navigation and member advocacy first (38%), followed by experience with system-run plans (36%). Tiered/preferred leaders led with employee and HR support (31%).
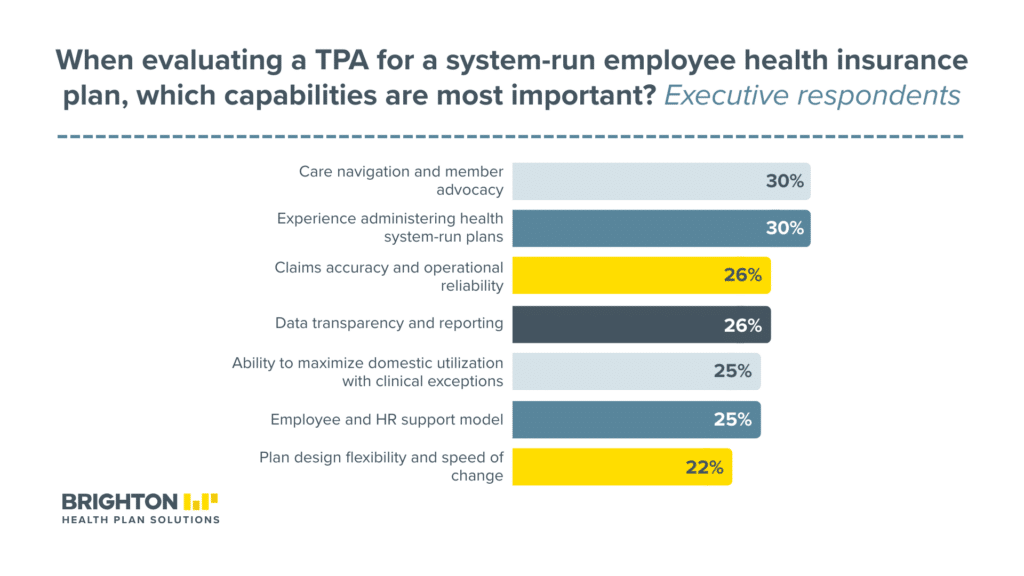
Across all network types, the top five TPA capabilities were care navigation and member advocacy (30%), experience with system-run plans (30%), claims accuracy and operational reliability (26%), data transparency (26%), and the ability to maximize domestic utilization while allowing clinical exceptions and geographic wrap networks (25%).
That last capability, balancing utilization with exceptions, is the operational expression of the strategic tension executives described in the utilization data. It’s where policy meets practice. And it’s a capability that only a TPA with deep health-system experience can deliver credibly.
Yet on the employee side, only 21% said they turn to their health plan administrator when they have questions. Most go to online portals (28%) or HR (24%). The TPA may be doing essential work behind the scenes, but employees don’t experience it as a resource they can reach. For a function that 99% of executives call important, that visibility gap is worth closing.
What’s next: priorities, barriers, and retention
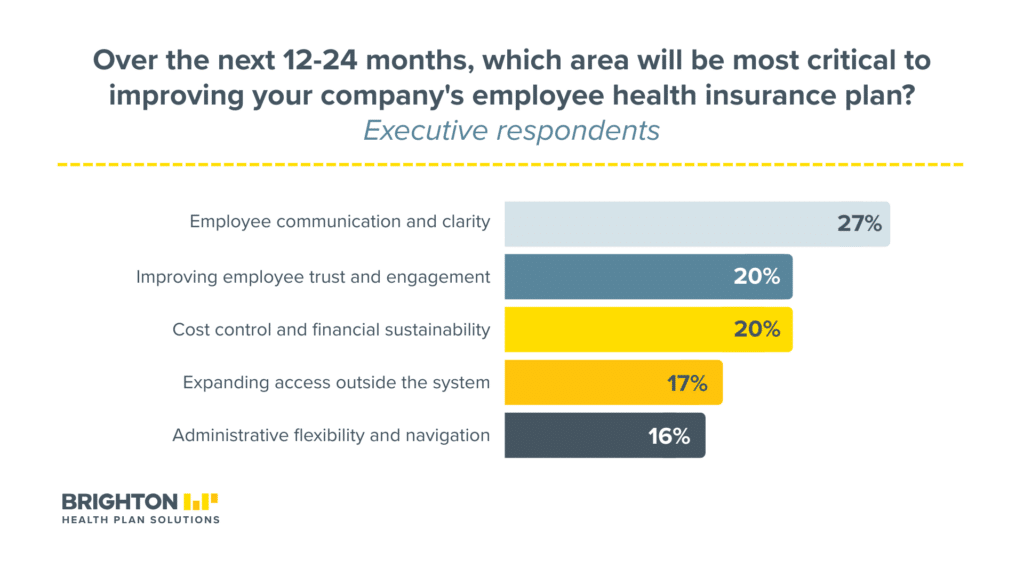
Executives know they need to act. When asked what they’d prioritize over the next 12 to 24 months, they put employee communication and clarity first (27%), followed by improving trust and engagement (20%) and cost control (20%). Expanding access outside the system came in at 17%, and administrative flexibility and navigation at 16%.
The barriers standing in the way are substantial and evenly matched. Three issues tied at 26% each: the pace of change in healthcare, the challenge of balancing utilization goals with employee needs, and the operational complexity of implementing meaningful change. Competing demands on organizational resources followed at 21%. Among in-system executives, balancing utilization versus employee needs ranked as the top barrier (28%), a reflection of the tension these leaders feel most acutely.
On the employee side, the retention data adds urgency. 37% of employees said the health plan has positively influenced their decision to stay with their employer, while 7% said it’s had a negative effect. That leverage skews younger: 44% of Gen Z employees said the plan positively affects retention, compared to 40% of millennials, 35% of Gen X, and 25% of boomers.
For self-funded health systems weighing whether administrative improvements are worth the investment, the generational trend is a clear signal. The workforce that will define the next decade of healthcare delivery cares more about the plan, and the experience behind it, than any group before it. The right TPA partner doesn’t just reduce friction. It protects the model.
“The data tells health system leaders something they probably already sense: the plan model isn’t what needs fixing,” said Michelle Zettergren, President, Chief Sales and Marketing Officer at Brighton Health Plan Solutions. “It’s the experience around it, the billing clarity, the referral process, the exceptions handling. Those are administrative capabilities, and they’re exactly where the right TPA partner makes the difference.”
Survey methodology
The Brighton Health Plan Solutions 2026 Self-Funded Health System Benefits Report was conducted in two parts in March 2026. The executive survey was administered by Censuswide among 250 U.S. C-level executives aged 30 and older at large, multi-site self-funded health systems (1,000+ employees), including in-system networks (42%), tiered or preferred networks (36%), and broad/open networks (22%). The employee survey was administered via Pollfish among 352 employees at U.S. health systems of comparable size who are currently enrolled in their employer’s self-funded health plan. The study examined both leadership strategy and employee experience across plan design, domestic utilization, administrative friction, TPA capabilities, trust, flexibility, and retention impact.